As healthcare professionals, most of us have heard of the ‘Resus Council’ and their regular updates, but who they are and what that means for us in practice is not always clear. This blog will explore who the Resus Council are, what the new 2025 changes include, why they matter, and how they impact us as healthcare professionals.
The 2025 update brings exciting developments, a more holistic approach, and greater community involvement. From teaching life-saving skills to children as young as four, to a new focus on First Aid as a core element rather than an addition to Basic Life Support, these changes mark an important step towards a more inclusive and proactive approach to saving lives.

The Resuscitation Council, often referred to as the Resus Council, is a committee of healthcare professionals who bring decades of expertise, research, and training experience to deliver life support courses and provide clinical guidelines for health and care professionals.
Formed in 1983, the Resus Council is dedicated to improving survival rates for both in-hospital and out-of-hospital cardiac arrests, working towards a future where everyone in society has the skills to save a life.
The Council produces clinical guidelines for all settings, along with training, guidance, and research on life-saving techniques. Their work extends beyond hospitals and classrooms, reaching communities, schools, and workplaces to help people at every level feel confident and prepared to act in an emergency.
By combining evidence-based science with accessible training, the Resus Council empowers healthcare professionals and the public to make a real difference when every second counts.
As mentioned, the Council produces a range of clinical guidelines for healthcare professionals to follow, both in and out of hospital. Some of the most well-known include:
These guidelines are reviewed and updated by the Council every five years to reflect the latest evidence, science, and research. Regular updates are vital to ensure that adults, children, and newborns receive the best possible care in all settings. They also allow us to analyse current statistics, compare outcomes over time, and recognise how improved guidelines directly contribute to better survival rates and the effective management of deteriorating patients and cardiac arrest.
Each update reinforces the importance of consistency and collaboration across all areas of healthcare. Whether in a hospital ward, ambulance, or community setting, these shared standards help every professional work with the same clear goal: to save lives through knowledge, confidence, and coordinated care.
This year, there are some very interesting changes to the guidelines. Here, we will look at each section to see what has changed and why.
‘Systems Saving Lives’ is part of the 2025 Resuscitation Council guidance that focuses on how joined-up systems can improve survival after cardiac arrest. It looks beyond individual skills and highlights how education, community response, emergency services, and hospitals must work together to make every link in the chain of survival stronger.
The update calls for a national approach to CPR and first aid, including mandatory training for schoolchildren, students, and drivers, starting from age four. It encourages annual refreshers and the use of interactive, technology-based methods to make learning more practical and consistent across the country.
The guidance also focuses on faster, more coordinated responses. Systems linking first responders with AED registries, and improved ambulance and hospital processes, are key to reducing time to CPR and defibrillation. Hospitals are urged to strengthen regional networks, improve post-arrest care, and support families who wish to be present during resuscitation.
Finally, the framework recognises that saving a life is only the beginning. It promotes long-term recovery and support for survivors and their families, with a focus on emotional wellbeing, rehabilitation, and involvement in future research and policy. In areas with fewer resources, local adaptation and international collaboration are encouraged to help raise survival rates everywhere.

The latest figures paint a clear picture of cardiac arrest across the UK. Each year, around 115,000 out-of-hospital cardiac arrests are reported to ambulance services, with resuscitation started in roughly 43,000 of these. Bystander CPR is given in about two-thirds of cases, showing how community response is improving, although defibrillator use is still low.
The average age for an out-of-hospital arrest is 65, with most happening at home and the majority occurring in men. Around 80% are caused by a cardiac problem. Paediatric arrests remain rare, with around 750–800 each year.
In-hospital arrests are less common, with about 12,755 cases each year. Around half happen on hospital wards, while the rest occur in emergency or critical care settings. Return of spontaneous circulation (ROSC) is achieved in just over half of adult patients, and around one in four survive to discharge at 30 days.
For adults, the most common rhythms seen are pulseless electrical activity (PEA) in 52%, ventricular fibrillation or tachycardia (VF/VT) in 18%, and asystole in 20%.
In children, there are around 200 in-hospital cardiac arrests each year, included within the overall total. Outcomes are generally better, with around 69% achieving ROSC and just over half surviving to discharge.
The 2025 updates place greater focus on early, person-centred conversations about emergency and future care, with increased emphasis on the ReSPECT form, which is now widely accessible across the NHS. The guidelines also highlight that families should be given the opportunity to be present during a CPR attempt if they wish, something that may not have been strongly emphasised in previous guidance.
Ethical training is now encouraged as part of resuscitation education, including through simulation. Embedding this within training gives clinicians the chance to develop confidence and preparedness for complex decision-making.
One of the biggest changes in this update is the push to start resuscitation education much earlier. Children as young as 4–6 years old should begin learning the basics of life-saving, with age-appropriate sessions built into the school year and continued every year as they grow. The goal is to make CPR and emergency response as familiar as any other essential skill.
For professionals, accredited training should be tailored to each person’s role, setting, and the patients they care for. Ambulance call handlers also play a crucial role and should receive specific training to recognise cardiac arrest quickly and guide callers through CPR over the phone.
There’s also a stronger focus on how we teach, not just what we teach. Modern methods like online learning, simulation, augmented reality, and artificial intelligence can make training more flexible and engaging. Gamified modules, real-time feedback, and structured debriefs turn learning into something active and practical, helping everyone feel more confident and prepared to save a life.

One of the biggest updates is found in adult basic life support. In the 2021 guidelines, the algorithm read: “Unresponsive, not breathing normally? Call 999 and ask for an ambulance.” The new version changes this sequence, now advising that 999 should be called straight away for any unresponsive person before checking breathing.
Once connected, ambulance service call handlers support recognition of cardiac arrest, give CPR instructions, and guide callers through using an AED. They also link to volunteer first responder systems and the nearest AED through The Circuit network.
Adult Advanced Life Support (ALS) continues to highlight the core priorities of early recognition, high-quality chest compressions, rapid defibrillation, and prompt treatment of reversible causes, with additional focus on correct pad placement and effective ventilation. For drug use, adrenaline remains recommended early in non-shockable rhythms and after the third shock in shockable rhythms.
In hospitals, early warning scores should be used to identify deteriorating patients quickly and help reduce in-hospital cardiac arrests through earlier recognition and intervention. Out of hospital, the focus is on identifying and managing cardiovascular risk factors, inherited conditions, and early warning symptoms. Data-specific debriefing after resuscitation is encouraged to improve team performance, and extracorporeal CPR may be considered in specialist centres when conventional CPR is unsuccessful.
There is also an update for cardiac arrest caused by drowning. Because these cases are usually triggered by hypoxia, the new sequence now emphasises giving five rescue breaths first, before starting chest compressions. This step was previously reserved for lifeguards but is now included for everyone providing resuscitation after drowning.
The latest guidance provides clearer instructions for AED pad placement. For adults, AED pads should still be placed as shown on the pads themselves, but particular care is now advised for the lateral pad. It should sit directly under the left armpit in the mid-axillary line, rather than lower down the side of the chest.
With regards to Advanced life support, if three shocks have been delivered without success, the guidance recommends considering repositioning the pad that sits near the right shoulder closer to the centre of the chest. This adjustment aims to ensure that the pads are positioned either side of the heart, improving the effectiveness of defibrillation.
These changes reinforce the importance of practical, real-world actions that save time, improve pad placement, and ensure oxygen delivery comes first when managing drowning-related arrests.
In paediatric resuscitation, the focus is on recognising unwell children early and acting fast using structured tools like the ABCDE assessment. Teams are encouraged to have clear activation processes so the right support is in place immediately. The guidance covers both basic and advanced life support, with clear advice on weight-based drug dosing, ventilation, shock management, and arrhythmias.
High-quality CPR and early defibrillation remain priorities, while extracorporeal CPR (ECPR) can be considered in specific cases where standard resuscitation isn’t enough. There’s also a stronger focus on prevention, early intervention, and keeping families involved throughout.
There are also key updates on resuscitation in special circumstances such as trauma, asthma, drowning, and hypothermia, along with clearer post-resuscitation care for children. These updates strengthen the whole chain of survival, from recognising reversible causes to providing the right management for each situation and ensuring structured follow-up to support recovery and long-term outcomes.
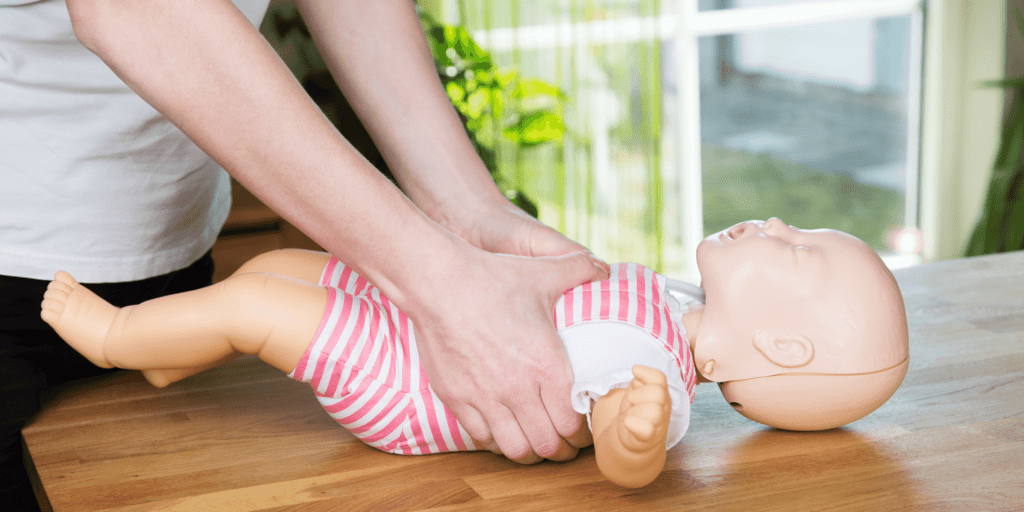
In the latest guidance, there are some important updates around paediatric life support techniques, especially for infants. For babies under one year, the preferred method is now the two-thumb encircling technique. This means placing both thumbs on the lower half of the sternum while the hands wrap around the infant’s chest to provide support. If this technique doesn’t allow for effective, high-quality compressions, the one-handed or two-handed method can also be used. For children over one year, either the one-hand or two-hand technique remains appropriate depending on the size of the child and the rescuer.
There’s also a slight update for choking infants. The recommendation still starts with five back blows, but if these don’t work, the next step is now five chest compressions using the encircling technique rather than the older two-finger method.
For AED use, the guidance has also changed slightly. If available, the paediatric mode should be activated for all infants and children weighing under 25 kg (around 8 years). For larger children and adolescents, the AED can be used in standard adult mode. If the device doesn’t have a paediatric setting, it should still be used in adult mode rather than delayed.
Pad placement has also been clarified:
This update specifies that the pad should now be placed just left of the sternum rather than centrally. These updates aim to make paediatric resuscitation more effective, ensuring high-quality compressions, safe AED use, and clearer steps for choking management across all age groups.
For newborns, the aim is to help babies transition safely at birth through a calm, coordinated team approach. Assessment now focuses on heart rate, breathing, tone, and response to stimulation rather than skin colour, as this can be unreliable and inconsistent. Airway management highlights the use of the two-person jaw thrust technique, supraglottic airways, and video laryngoscopy where available. Adrenaline is given every four minutes, and bicarbonate has been removed from practice.
The guidance also extends beyond hospitals, covering home births, ambulance care, and unexpected deliveries. It includes practical steps for maintaining temperature, managing the airway, gaining vascular access, and ensuring safe transfer, with telemedicine support where possible.

For the first time, first aid has been introduced as its own chapter, recognised as the first link in the chain of survival. It’s described as help provided by anyone, in any setting, before professional help arrives. The focus is on early action, keeping the scene safe, and following a clear, structured approach such as ABCDE. First aiders are encouraged to call 999 promptly, use only equipment they’re trained to use, and focus on reassurance and safety until professional help takes over.
This new chapter gives clear and practical guidance for common emergencies including choking, severe bleeding, drowning, chest pain, asthma, anaphylaxis, low blood sugar, overdose, stroke, and trauma. It also outlines simple, step-by-step actions such as placing someone in the recovery position, using tourniquets, adrenaline pens, and naloxone where appropriate. Environmental emergencies like heat stroke, hypothermia, snake bites, and concussion are also included.
Training is encouraged to be inclusive, accessible, and relevant to the needs of different communities, including rural and low-resource settings. It also aims to build confidence and reduce the hesitation or fear that can stop bystanders from stepping in. This new addition highlights that everyone has a role to play in saving a life, placing first aid firmly at the heart of the UK’s resuscitation framework.
These updates build on what already works while refining how we teach, respond, and support each other in emergencies. Each change is designed to strengthen confidence, consistency, and survival outcomes across every stage of care.
But what does this actually mean for health professionals? The changes themselves aren’t overly extensive, but they do bring clearer guidance and stronger emphasis on what we already knew, showing the importance of actually putting that knowledge into practice. The aim is to improve recognition of the deteriorating patient and strengthen how we identify and respond to cardiac arrest. With these updates, the hope is that more people will feel confident in delivering CPR effectively, leading to fewer deaths and improved survival rates.
So, what does all of this actually mean for us as healthcare professionals? In simple terms, it’s a reminder of how vital our role really is. These updates aren’t about changing everything we do, but about reinforcing what already works and adapting to the changes highlighted. Recognising when a patient is deteriorating, acting early, and feeling confident in our response are key.
It’s also about keeping our knowledge fresh, supporting each other as a team, and involving families where we can. Whether it’s teaching basic skills, leading a resus call, or noticing when something isn’t right, these changes encourage us to keep improving so we can give every patient the best possible chance.
The Resus Council UK encourages all organisations to prepare for implementation of the new 2025 guidelines over the next 12 months. Updated training materials and manuals will be released from January 2026. Health Academy will also be launching our updated course designed to help you refresh your skills and stay aligned with the latest guidance. Keep an eye out for these updates to ensure your knowledge remains current and your practice reflects the most up-to-date standards.

Changes to the guidelines, updated statistics, and the introduction of new sections are exciting, important steps that move resuscitation practice forward. They remind us that healthcare is always evolving and that staying current is part of our responsibility to both patients and families. These updates encourage a more proactive, person-centred approach, where prevention, education, and confidence go hand in hand. By keeping our skills and understanding up to date, we not only improve outcomes but also help create a culture where everyone, from healthcare professionals to the public, feels empowered to save a life.