The release of the new GP contract early in 2023 highlighted that some changes are coming to the vaccination schedules for some diseases. One of which is shingles (the other is HPV but that’s for another blog). Are you ready for the transition? The Shingles vaccination changes could be quite complicated. Read on to learn more about the background and the changes to expect.
The aims of vaccination programs in the UK are not all the same. Of course, the holy grail is to eradicate the disease completely so we don’t even need to give a vaccine. This has happened in a handful of cases, with Smallpox being a very notable example. Smallpox is not a disease we have to worry about anymore – largely because of the wonders of vaccination. However other pesky orthopoxviruses are still sneaking about. Enter: Monkeypox, which you have probably seen a lot about in the news this year.
Sometimes the vaccine program is about keeping diseases at bay and maintaining good levels of herd immunity while they are still around lurking either in small cases or in other countries. For example, one of our arch enemies, polio. We have not had a case in the UK for many years (since 1984) but because it exists in other areas of the world it’s best to keep it there on the program to keep the antibodies circulating, and protect our most vulnerable. The WHO is aiming to eradicate this one too if they can maintain successful polio vaccination campaigns across the world. Read more about the GPEI Strategy 2022-2026 here.
But, some vaccines are not about herd immunity, or protecting the country from spread of disease. They are more concerned with protecting the individual from themselves.
Shingles vaccine is a vaccine against misery and suffering. It is not really a disease that can be ‘caught’ as such. The virus that causes it lives inside the individuals’ nerves and re-emerges just at the point where you really really LEAST need it (stressful situations like house moves, exams, divorces, and ill health, for example).
Wel, it begins with the chicken pox virus. And, this disease, as we all know, CAN be caught. So, you catch chicken pox meaning you contract the Varicella-Zosta Virus (VZV). Then the virus remains dormant on the nerves. And then it pops up again as shingles when you are stressed, old, or ill. It’s a real nightmare. Burning tingling skin over the site of the nerve it’s residing in; rash, pain, and pure misery. Most of us will have had chicken pox at some point – there’s a 95% chance if you have been a room with someone who’s got it (and you are non-immune) that you’re going to get it. So, shingles risk in later life is HIGH. Roughly 1 in 4 of us will experience it at some point.
At the moment the UK vaccination program for shingles concentrates on two factors;
And these two are unfortunately not necessarily well-correlated. It probably is time for the shingles vaccination changes.
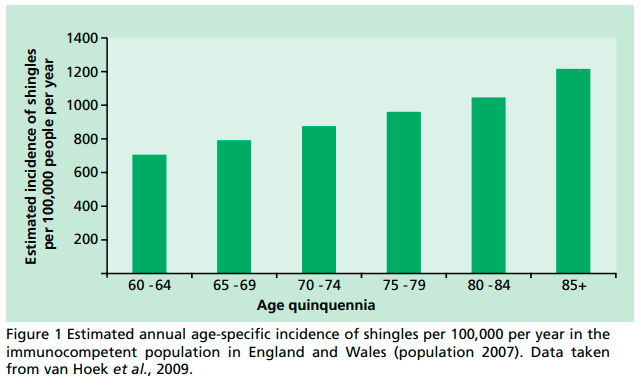
As you can see from the graph (borrowed from the Green Book), it’s clear that the older you are, the worse your chances of experiencing shingles. However, we have been vaccinating solely the 70-79 age groups. This is not because your chances of getting shingles drops off when you hit 80. Quite the opposite in fact. The reason is because the vaccine is simply not as effective for them. And younger age groups? Well, it’s not been considered as cost-effective to vaccinate those who are better able to tolerate the disease because of their youthful antibodies.
There are two vaccines we use in the UK, both of which have been available privately if people wish to have them out of the NHS 70-79 funding bracket. The licence for Zostavax is from 50 and Shingrix is from age 18.


Things are changing from an NHS funding point of view though relating to Shingles vaccines. Firstly, Zostavax is being discontinued and Shingrix will be the primary (and only) vaccine in use on the program. And secondly, the age ranges are changing. In addition to this, the intervals between doses of Shingrix are changing too. All this is going to be implanted gradually from September 2023. Read all about it here in the new GP contract for 2023-2024.
Zostavax has been the primary vaccine of choice for some time. In 2018 the JCVI announced that they were happy that another vaccine- Shingrix -was effective and cost-effective. They hence recommended its use in the NHS Shingles Programme for individuals for whom the live vaccine, Zostavax, was contraindicated. This welcome change was implemented in the programme in September 2021. Finally! Those who were most vulnerable could be vaccinated with an inactivated option now on the cards.
But it was not long after the initial discussions about Shingrix, in 2019, that the JCVI had started to talk about entirely replacing Zostavax with Shingrix and considering starting shingles vaccines from a younger age.
Then the pandemic hit and focus became COVID-19. And no one really knew if anyone would live long enough to be worrying about shingles for a bit.
But now, in 2023, Zostavax is finally retiring after many successful years of service. To be replaced with its inactivated colleague, Shingrix.
Shingrix, which people have known as two doses, 8 weeks apart for all this time, will then have a longer interval between the two doses. It will also be given from age 50 to immunocompromised people (with an 8-26 week interval). AND, not only that, the immunocompetent cohort age criteria is being expanded from age 70 right down to age 60 (26-52 week interval). The upper age limit seems to be the only thing staying the same for the immunocompetent group (80). The immunocompromised groups will have no upper age limit.
First, we will have to use up all the left over Zostavax. Would be a shame to waste it when the shingles vaccination changes start to be implemented. This will continue in the 70-79 age groups for as long as it lasts.
Then, there will be two five-year stages to sort all this out.
Additionally, we will need to catch up those who are newly eligible when September comes around. And all those who are immunocompromised over 50 will be a priority and there will be lots of catching up to to. The aim of the programme is to vaccinate ALL over 50’s in this group within the first year.
This phased approach will likely amass some confusion along the way so make sure you stay up to date with the guidance as it comes in. There is likely more detail to come about the exact logistics of the shingles vaccination changes as we go along. Keep an eye out here.
Of course, not to mention that all this will be happening during the madness of flu season while everyone is still getting to grips with which influenza vaccines to give, and to whom, at the same time.
One thing that has also been on my mind is around the chicken pox virus. Could the expansion of age ranges be setting the scene for introducing the chicken pox vaccine to the routine childhood schedule?
The implications of adding chicken pox vaccine for kids are that it could potentially have a knock-on effect with shingles. When children catch the disease, adults are naturally boosted by being around them as a result of the natural effects of the disease itself. This keeps the immune system prepared for holding off a shingles appearance. If we vaccinated kids, would we see more cases of shingles in adults if children consequently stop getting sick with chicken pox and shedding their virus particles everywhere? Yet, if we keep it the same, what are the ethical concerns with allowing our children to catch diseases naturally so we can benefit from them as ‘living boosters’?
It’s a complicated decision that the JCVI have visited a few times and not come to a conclusion on just yet. There is still more modelling to be done. However, they have consulted with their counterparts in the USA where there has been a childhood chicken pox programme for some time. Read all about it here. Maybe this is a topic for another blog sometime.
I’m intrigued to see how this all pans out.
The new Green Book Chapter was published on Monday 17th July and is for use from 1 September 2023. Have a read now!
Good luck with the shingles vaccination changes when switchover starts unfolding. And come and join us on an immunisation course before then so you are nice and prepared!
We also have an online Shingles Short Course available here.